

Esophageal Cancer is deadly!
Esophageal Cancer is deadly!
But reading this article is a call to action and may save your life


I wanted to write about gastroesophageal reflux disease (GERD) and it’s association with esophageal cancer to hopefully scare you into taking action. In a systematic review of 15 epidemiological studies, the prevalence of gastroesophageal reflux disease (GERD) was found to be 10 to 20 percent in the Western world. The incidence in the Western world was approximately five per 1000 person-years or 0.5 percent per year.
In the most general terms, GERD is a condition that develops when the reflux of gastric (stomach) contents causes troublesome symptoms. The classic symptoms include heartburn and regurgitation. Regurgitation is defined as the perception of flow of refluxed gastric content into the mouth. People typically regurgitate acidic material mixed with small amounts of undigested food. Other symptoms of GERD include dysphagia (difficulty swallowing) and chest pain. Dysphagia is common in the setting of long-standing heartburn. The presence of dysphagia mandates prompt workup. Extraesophageal symptoms can include chronic cough, hoarseness, and wheezing. In a recent population-based survey in the United States, 22 percent of respondents reported that they had heartburn or regurgitation within the last month while 16 percent reported regurgitation. In other words, GERD is pretty common!
GERD is classified based on the appearance of the esophageal mucosa (lining) on upper endoscopy (EGD) into the following:
Erosive esophagitis — Erosive esophagitis is characterized by endoscopically visible breaks in the distal (furthest from the mouth) esophageal mucosa (lining) with or without troublesome symptoms of GERD.
Nonerosive reflux disease — Nonerosive reflux disease or endoscopy negative reflux disease is characterized by the presence of troublesome symptoms of GERD without visible esophageal mucosal (lining) injury.
The diagnosis of gastroesophageal reflux disease (GERD) can often be based on clinical symptoms alone in patients with classic symptoms such as heartburn and/or regurgitation. Other disorders need to be excluded before attributing the symptoms to GERD. As an example, unexplained chest pain should be evaluated with an electrocardiogram and exercise stress test prior to a gastrointestinal evaluation.
Now the part that may save your life!…….The causal relationship between GERD and esophageal adenocarcinoma has been clearly established.
This basically means that the far majority of people who are diagnosed with esophageal adenocarcinoma (CANCER) have pre-existing GERD. I want to share an important thought that is generally agreed upon by most dedicated esophageal surgeons….and that is that there is a parallel rise in the use of OTC medicines for GERD and the rise in the incidence of esophageal adenocarcinoma (CANCER). The reason for this is very simple. In people with GERD who have esophagitis, they actually have what is called duodenogastric reflux. That means that the gastric acid (stomach) is mixed with the non-acidic bile secretions from the duodenum and pancreas. The gastric acid component causes the “ouch” and tells you something is going on and that your esophageal lining is being damaged, and it is the duodenogastric contents ,which when mixed all together, lead to esophageal adenocarcinoma. Proton Pump Inhibitors (PPIs) which includes omeprazole and lansoprazole and H2 blockers including Tagamet, Pepcid, and Zantac “neutralize” the acid and get rid of the “ouch” but do not change the duodenogastric reflux which causes the damage.
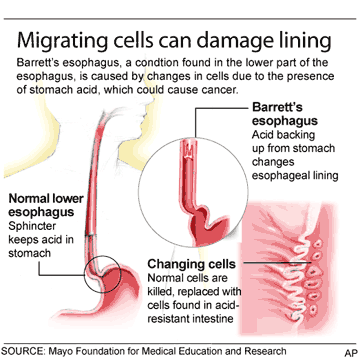
In medical terms, the duodenogastric reflux can lead to Barrett’s esophagus (BE), which is defined as intestinal metaplasia (IM) of the esophageal mucosa. This is a known precursor of esophageal adenocarcinoma (CANCER) and is thought to result from chronic GERD in genetically susceptible individuals.
Esophageal adenocarcinoma (CANCER) is a dreaded disease with a poor prognosis, largely due to the advanced stage at which it typically presents. While still a relatively uncommon malignancy, it has been increasing in incidence over the past 50 years in the United States (US) and Western Europe. Data from the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) Program estimate that a total of 20,640 new cases of esophageal cancer will be diagnosed in the US in 2022, most from esophageal adenocarcinoma, constituting 1.1% of all new cancer cases. Sadly, the 5-year relative survival of esophageal cancer between 2012 and 2018 was only 20.6%. While this survival rate is poor, it represents an improvement from 50 or more years ago when fewer than 5% of patients diagnosed with esophageal cancer survived more than 5 years. While the epidemiology of esophageal cancer has shifted since the 1970s, from a predominance of cases of esophageal squamous cell carcinoma to the majority now being esophageal adenocarcinoma, the reasons behind the steady improvement in prognosis are multiple. An increased frequency of detection and treatment of esophageal cancer at earlier stages, however, undoubtedly plays a role in its better overall survival.
Upper endoscopy is not required to make a diagnosis of GERD. However, upper endoscopy can detect esophageal manifestations of GERD. Upper endoscopy is indicated in patients with suspected GERD to screen for Barrett’s esophagus in patients with risk factors. Risk factors for Barrett's esophagus include:
Duration of GERD of at least 5 to 10 years
Age 50 years or older
Male sex
White individuals
Hiatal hernia
Obesity
Night-time reflux
Tobacco use (past or current)
First-degree relative with Barrett's esophagus and/or adenocarcinoma
The simple take home message is that if you have GERD symptoms for more than 3 months, you should talk to your family doctor or call a gastroenterologist. For further guidance or medical advocacy, please go to PaladinMDs because “it’s like having a doctor in the family.”
My last upper endoscopy biopsy on August 2nd came back “Barrett’s mucosa, negative for dysplasia. Reflux esophagitis.”
Recommendation was to continue current course of PPI‘s and repeat upper endoscopy in one year.
Can I take comfort in the fact that the result was negative for dysplasia? I have to take generic Tums for breakthrough GERD pain.